Where cop cars double as ambulances
In Philadelphia, police often race shooting victims to the hospital rather than wait for paramedics. Experts in trauma and policing say more cities should consider it.
This story was reported by the Trace with NBC Philadelphia.
Ian Hirst-Hermans lay on the ground, bleeding from a gunshot wound to his chest. He had been shot after leaving a house party just after 2 a.m. Within seconds, as he remembers, a police car came racing down the one-way North Philadelphia street in the wrong direction. Two cops jumped out and, with the help of his friend, lifted Hirst-Hermans into the back.
Blood pooled beneath the 20-year-old on the hard plastic backseat. He was sure he was going to die. Then from the front of the car came a calming voice. One of the officers was asking him questions about his college classes, telling him he was going to make it. Hirst-Hermans’ last memory of the drive was the siren of an ambulance blaring past and one of the officers saying, “There goes your ride.”
Had he been shot in another city, Hirst-Hermans might have died. The bullet hit a major artery in his chest, and he’d lost a lot of blood. A surgeon later told him that he’d made it to the hospital with less than a minute to spare.
Among cities with the highest rates of homicide, Philadelphia is the only one where police routinely rush gunshot and stab wound victims to the nearest trauma center instead of waiting for an ambulance. The practice — known as “scoop and run” or “scoop and go” — is deeply entrenched among the city’s law enforcement officers, who focus their patrol in areas with the highest instances of violent crime and, as a result, frequently beat EMS to crime scenes. “The sense has always been, get that person to the hospital quick,” says John Stanford, a captain and 16-year veteran of the Police Department. “It’s just something you do.”
Last year, a third of Philadelphia’s 1,223 shooting victims were delivered to a city trauma center in the back of a police cruiser or wagon. At Temple University Hospital, the busiest hospital for gunshot patients in the state, about 70 percent of victims of penetrating trauma arrive by police vehicle or private vehicle, or simply walk in.
Though Philadelphia police receive basic training on treating gunshot wounds, including how to apply a tourniquet, most of the victims they transport receive little or no medical care until they’re through the hospital doors. The practice challenges how most people think victims should be cared for. Yet trauma doctors in the city are effusive about scoop and run, and believe it saves lives. “Patients often survive the initial gunshot, but unfortunately a large number of them bleed out fairly quickly, within seconds and minutes,” says Marcin Jankowski, the head of trauma and surgical critical care at Hahnemann University Hospital, one of the city’s eight trauma centers. Doctors say the faster these patients can get to a trauma center, the better their chances at survival.
“Philadelphia is unique. The police have definitely taken ownership of getting patients to us as quickly as possible,” he adds.
Beyond its lifesaving potential, some say, scoop and run could enhance public safety in communities with broad distrust of police. When officers lift victims into the backseats of their cars, they become true first responders, shifting roles from enforcer to guardian, from soldier to protector.
As intuitive as scoop and run is among Philadelphia cops, police departments in other cities have little appetite for the practice. They argue that cops have other important responsibilities, such as solving crimes; they lack the advanced medical training required of EMTs and paramedics; and there could be liability issues when victims don’t survive.
In certain circumstances, police in other cities already embrace scoop and run, such as during mass shootings and when their colleagues are wounded.
Research suggests cities should consider innovative transport methods for all shooting victims. A recent national study found that the rate of gunshot victims who died en route to the hospital quadrupled between 2007 and 2014. “Their injuries are so severe that by the time they come to us, it’s very difficult to save their life,” says Joseph Sakran, the study’s author and a trauma surgeon at Johns Hopkins Hospital in Baltimore.
After the two Philadelphia cops delivered Ian Hirst-Hermans to Temple’s trauma center that night eight years ago, surgeons got to work, removing an artery from his thigh to replace the destroyed one in his chest. He awoke the next day shaken. But his mood brightened when the two officers who scooped him came to visit. One joked that Hirst-Hermans needed to hurry up and get well so he could clean the blood out of their car.
Hirst-Hermans texts the officers every holiday season to thank them for getting him to the hospital. A few years ago, he had their last names tattooed in thick black cursive beneath his clavicle. “They’re my heroes,” he says. “I’m eternally grateful to those guys.”
In Philadelphia, scoop and run is such a long-held tradition that many officers can’t imagine their jobs without it. “It was just something that was understood, that getting the person to the hospital was part of your duties,” says Kevin Bethel, a retired former deputy police commissioner who joined the department in the mid-1980s.
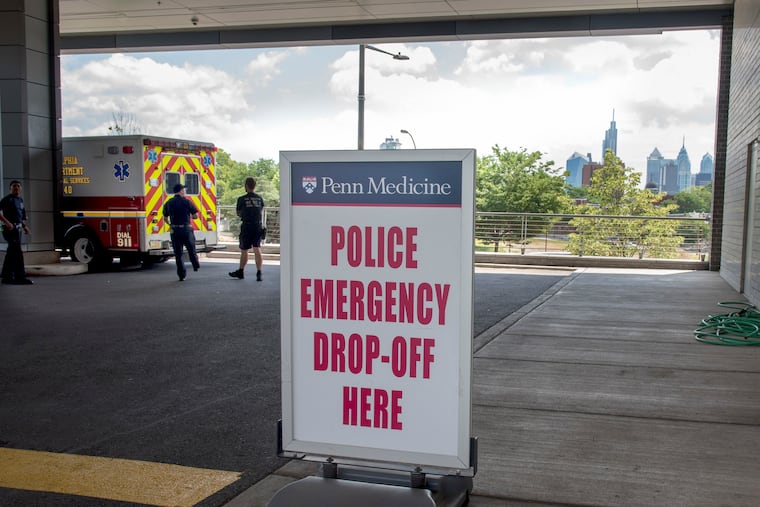
Last year, police drove 408 gunshot victims to Philadelphia trauma centers, according to the Pennsylvania Trauma Systems Foundation, the state’s accrediting agency for trauma centers. In the last decade, police scoop and runs of gunshot victims have nearly doubled, even as shootings have remained fairly level. The practice has become so common that Penn Presbyterian Medical Center, a Level I trauma center, recently designated a drop-off lane for cop cars.
Steven Davidson, the city’s former EMS medical director, helped lead one of the first systematic evaluations of scoop and run, a 1995 study that compared mortality rates of assault victims transported by police to those driven by medics. The researchers found no significant differences in survival. A year later, the Philadelphia Police Department formalized its policy, which instructs officers to transport gunshot and stabbing victims and not wait for EMS. In the years since, research on the city’s practice has reached similar conclusions.
The studies are far from perfect — they did not control for transport times or medical interventions in the field — but many clinicians interpret the findings to mean police transport is safe for patients, and in some cases advantageous.
One citywide study included a subset of people severely injured by gunshots. Compared with those transported by EMS, patients ferried by police had higher rates of surviving their wounds.
Philly police interviewed by the Trace and NBC Philadelphia consider scoop and run a natural part of their role. The only protective gear they carry are medical gloves; they expect to get bloody. “We don’t join the Police Department to watch people die,” says Stephen Clark, a captain for the 24th District, which has seen some of the highest numbers of shootings in the city.
To residents on the other end of a scoop and run, its logic may be less obvious. Rather than being tended to by trained EMTs and paramedics with a range of medical supplies and equipment, they are hoisted into the back of police cars, where they may not even receive direct pressure to their wounds, not to mention a buckled seat belt. “You’re hitting bumps, you’re bleeding, your body’s going all over the place,” says Terry Starks, who was transported by a cop after being shot five times in 2002. Philadelphia officials say that, to the best of their knowledge, neither the Police Department nor the city has been sued over police transport of victims. The Trace identified two civil lawsuits brought against the city by individual families who alleged the actions of police — including transporting and not applying pressure — contributed to their sons’ deaths. Neither went to trial.
According to some trauma doctors, the lack of medical intervention that victims receive during the typical scoop and run is part of what makes the practice beneficial. Advanced procedures such as breathing tubes and IV fluids, although helpful for certain kinds of patients, may actually do more harm than good for shooting and stabbing victims in urban areas.
“I’d love to debunk the myth that you need a person on the scene who has all this advanced medical training and that is going to make the difference for this specific kind of injury,” says Elliott Haut, a Johns Hopkins trauma surgeon. For a presentation he gives at conferences, he shows a slide that asks what’s the best fluid to give victims of penetrating trauma. Then he clicks to the next slide, which reads “diesel fuel.” Haut says, “Yes, you’re going to get less medical care on the street and in the back of the car, but I’m OK with that because the shorter time is going to make a difference.”
While several police departments have policies permitting their officers to conduct transports — including Cleveland, Chicago, Detroit, and Stockton, Calif., — none of the 13 cities surveyed for this report reported transporting victims on a regular basis.
Cleveland residents would not benefit from “a Philadelphia-style police transport program,” wrote a representative of Cleveland’s paramedic and EMT union in a recent op-ed, pointing out that Philadelphia has five adult Level I trauma centers all within close proximity, while Cleveland has just two on opposite sides of town.
Neighborhoods with disproportionately high gun violence are often the same places where residents fear and distrust the police, making them skeptical of scoop and run. “I can tell you about times where there’s a victim in the back of my car and every other word is an expletive to us. ‘I’m not snitching, punk-ass cop,’” says Stanford, the Philadelphia captain. “And I’m still driving like a bat out of hell to get this guy to the hospital to save his life.”
Some scoop and run proponents hypothesize that having an officer spirit you or a loved one to the hospital at a life-or-death moment might have an unexplored power to help mend trust between police and residents of high-crime neighborhoods. “Being able to say to the community, here are instances when police have saved the lives of these frequently young victims of gun violence, I think is another justification for doing this,” says Jim Bueermann, president of the National Police Foundation, a policing innovation nonprofit.
Bueermann speaks about scoop and run in existential terms. “On this issue,” he says, “the Philadelphia Police Department is directly connected to the spirituality of policing” — the point of police work, to protect and serve. “The things cops see day in and day out are frequently negative,” he adds. “Having an opportunity to save a life in the performance of their duties gives officers a tremendous emotional boost.” Still, he thinks that for other cities to adopt scoop and run will require buy-in not just from police chiefs, but also city managers, city attorneys, mayors, and other local leaders.
A few weeks ago, Penn Medicine hosted a conference at which clinicians held a debate and panel on police transport for trauma victims. Dan Holena, a trauma surgeon at Penn Presbyterian Medical Center, conceded that scoop and run would probably not work in certain places, such as cities with a lower concentration of trauma centers. “I can think of a half a dozen major U.S. cities where this could work and really should work, and the only reason that it’s not are things” — such as local policies, culture, and legal concerns — “that really don’t have to do with care of the patient.”
Officials in Camden decided to take a chance on scoop and run a few years ago. The chief of the Camden County Police Department, Scott Thomson, hoped it would help build cops’ credibility among residents.
At first, some officers were wary. “Anytime you implement something new and fundamentally different, there’s hesitation and some folks resist,” Thomson says. But he says they came around, and now his officers scoop about one in every five of Camden’s gunshot and stab wound victims. In a few cases, officers even transported victims who were shooting directly at them.
“The streets are always watching,” Thomson says. “And they see your behavior, and actions speak far louder than words.”