Why so many women choose silicone implants for breast reconstruction
Valerie Wakefield is 66, old enough to remember the 1990s, when legions of women worldwide contended that silicone gel breast implants made them horribly ill.
Valerie Wakefield is 66, old enough to remember the 1990s, when legions of women worldwide contended that silicone-gel breast implants made them horribly ill.
Nonetheless, the Mount Airy nurse chose to replace her left breast with a gel implant after her mastectomy three years ago.
She is not unusual. The device - once the subject of a government ban and a product-liability debacle - is now the preferred breast-reconstruction method. Of 106,000 restorative surgeries performed last year in the United States, more than 80,000 involved silicone-gel implants, according to the American Society of Plastic Surgeons.
The reasons are complex, but two factors are clear.
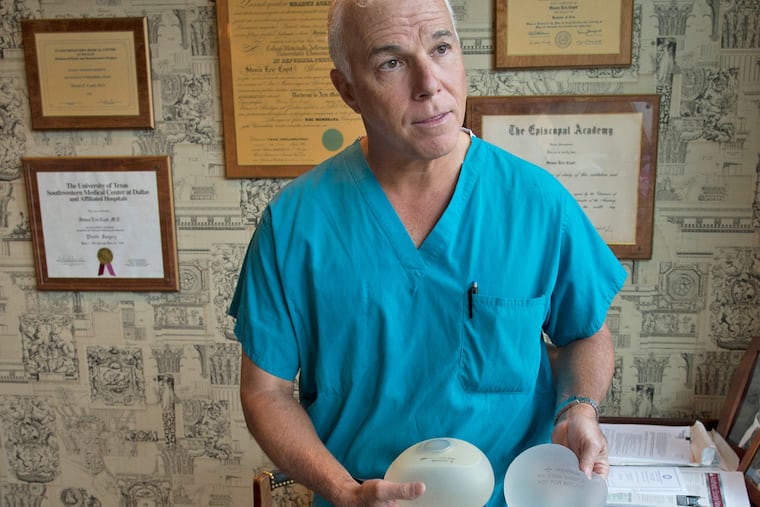
"More patients are candidates for implants because we have better silicone implant technology, and better mastectomy techniques," said Steve Copit, chief of plastic surgery at Jefferson University Hospital.
Saline-filled implants tend to look and feel less natural than the gel-filled versions. Fashioning a breast using tissue from another part of the woman's body - favored for long-term satisfaction and appearance - is a far more invasive, difficult surgery.
Wakefield, who recently shared her hard-earned wisdom at a reconstruction seminar sponsored by the advocacy organization Living Beyond Breast Cancer, summed up her thinking: "I was going to get the longer procedure where they would take tissue from my abdomen. But I decided I didn't want to be in surgery for 8 to 10 hours. I knew the recovery period would be prolonged. If I was 30 or even 40, I might have gone for it. I was a little concerned initially about silicone rupturing or leaking. But I did some research and I felt confident. I've had a very good result."
Debunking claims
Silicone-gel implants for breast enlargement came on the market in 1962, before the Food and Drug Administration had authority to regulate them.
In 1992, with more and more women blaming gel implants for autoimmune and neurological diseases, the FDA restricted the device to women willing to participate in studies - including a large study for reconstruction patients. (Saline-filled implants were not restricted.)
As a deluge of lawsuits upended the implant industry, independent expert groups began reviewing the scientific evidence, looking for links between gel implants and diseases, including breast cancer.
The consensus: Although implants had problems with rupture, deflation, breast hardening, infection, and pain, they did not cause diseases.
"The research debunked those claims," said Kamakshi R. Zeidler, a reconstructive plastic surgeon in Campbell, Calif. "That data is very strong and gives us as surgeons confidence in recommending implants to women."
In 2006, the FDA lifted its restrictions, ruling that the manufacturers Allergan and Mentor provided "reasonable assurance" that their products were safe and effective.
Long before that, however, more women were opting for gel implants, which drove an increase in reconstructive surgeries, studies found.
For example, an analysis of a private insurance database by MD Anderson Cancer Center researchers showed that in 2007, 63 percent of mastectomy patients underwent reconstruction, up from 46 percent in 1998 - the year a federal law required insurers to cover reconstructive surgery. Over that period, surgeries using patients' own tissue fell by more than half, to 25 percent, while gel implants saw a corresponding increase.
The shift "is perhaps the most important change in post-mastectomy breast reconstruction," Memorial Sloan Kettering researchers wrote this year in the Journal of Surgical Oncology.
Some complications still
That's not to suggest implants have become problem-free. Both Allergan and Mentor have patient booklets that warn, "Breast implants are not lifetime devices." The lengthy documents explain the nature and frequency of complications such as breast hardening, rupture, and implant removal or replacement, based on the studies that led to approval.
Still, the latest generation of the device has relieved some basic flaws.
"The outer shell is thick and strong and resists rupture," said Copit at Jefferson, demonstrating by closing his office door on a Mentor implant.
Implant innards are now made of a "cohesive" gel that holds its shape. If the pouch rips, the gel stays in place. Older implants, in contrast, had a gloppy goo that could ooze out of a hole, creating disfiguring lumps or migrating to other parts of the body.
Although women are supposed to have MRIs every few years to check for rupture of cohesive gel implants, few do so because insurance won't pay for it, doctors say.
"A lot of women are walking around with a 'silent' rupture and don't even know it," Copit said.
Experts cite other advances that have fueled the shift to gel implants:
Mastectomy has become less disfiguring. Surgeons now aim to preserve the breast skin, often with the nipple and areola. This is a particular boon for the growing number of women opting for double mastectomies, often because they have a hereditary risk of breast cancer.
Implants come in a vast array of sizes and shapes to suit more bodies. So do "expanders," the temporary pouches that are put under the chest wall muscle after mastectomy and then, over several months, gradually inflated with saline to create space for the actual implant.
Engineered tissue, made from donated human skin, is now routinely added to the chest wall muscle for better healing.
Improved surgery
While implants have gotten better, reconstructive surgery using patients' own tissue also has improved.
Traditionally, flaps of skin, fat, and muscle from the abdomen were maneuvered into position, while remaining tied to their original blood supply.
"Now we detach and move the blood supply, then use microsurgical techniques to reattach it" to vessels in the chest, explained John G. Fernandez, a reconstructive plastic surgeon at Cancer Treatment Centers of America. "That preserves the integrity of abdominal muscles. There's less pain, a faster recovery, and less risk of hernias."
For patients who need radiation to treat their cancer, tissue reconstruction has another advantage.
It "tends to tolerate the damaging effects of radiation the best," explained Lankenau Medical Center radiation oncologist Marisa Weiss, founder of the patient information site breastcancer.org.
Some studies suggest that declining insurance reimbursements have shaped the shift toward implant surgery, which takes only about two hours, a quarter of the time needed for tissue reconstruction.
In any case, a federal law passed late last year, the Breast Cancer Patient Education Act, aims to make sure that women get information to understand their rights, as well as which restorative options best meet their needs.